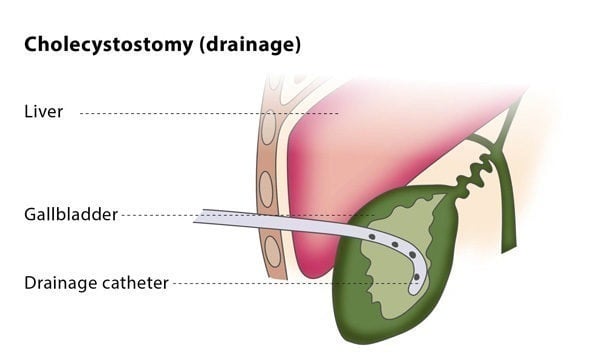
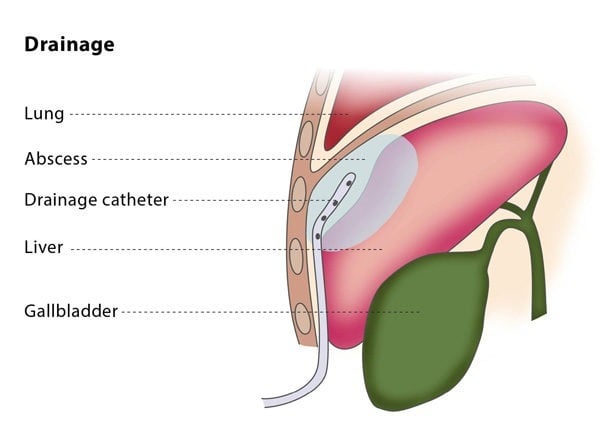
Image-guided percutaneous drainage involves using a catheter (a thin tube) to drain an abscess or a collection of fluid or air under image guidance. The interventional radiologist will insert a flexible catheter through a small cut in your skin and will guide the catheter to the collection of fluid or air. The fluid or air will then be collected in a drainage bag.
Drainage catheters are available in a variety of sizes, shapes and types. The interventional radiologist will choose the catheter according to the type of fluid, along with other factors.
If you are on any medication that prevents blood clotting, you will stop taking it before the procedure, if possible.
You should not eat anything for at least four hours before the procedure starts. You may be asked to fast for longer, depending on the puncture and difficulty of your particular case. Before the procedure, the interventional radiologist will usually place a needle in your vein to make access easier during the procedure.