
The goal of tumour ablation is to destroy the tumour without using surgery. Whether you are suitable for this procedure depends on the size and location of the tumour as well as your clinical situation.
If your case is critical, you may need to undergo additional stenting of these vessels to avoid restricting the blood supply.
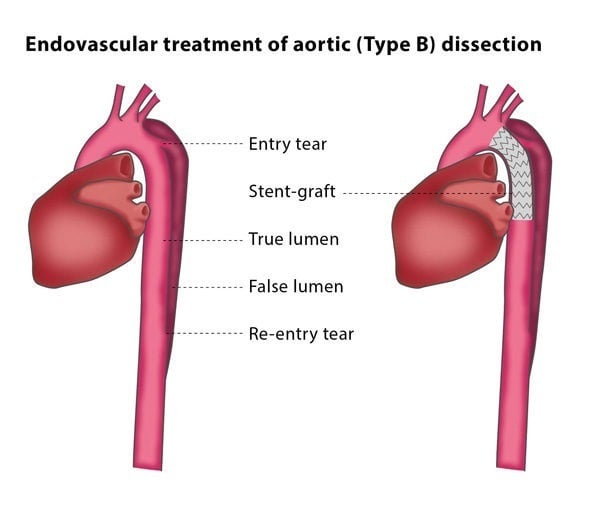
If a stent graft is not enough to decompress the false lumen, you may be advised to have a procedure called fenestration of the intimal flap. This means that a hole will be made in the membrane between the true and false lumens to equalise the pressure between them. The interventional radiologist will create a connection between the lumens using a needle and positioning a wire through the puncture site. They will then widen the hole using a tiny balloon and may implant a stent to keep the connection open.