Before the procedure, the interventional radiologist will outline the obstruction with contrast material under X-ray. You will have a local anaesthetic in your throat and be under mild sedation for the procedure. The interventional radiologist will introduce a device containing a wire and a catheter through your mouth and to the blockage in your gullet or small intestine. After the narrowing has been reached with the wire, a tiny balloon will be introduced and will slowly expand to dilate the area around the blockage.
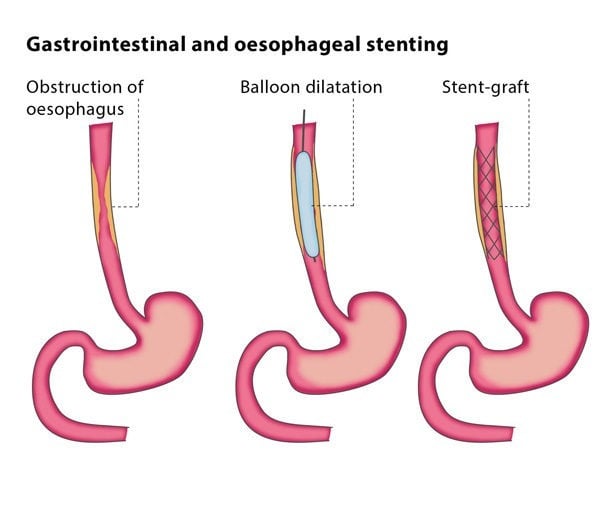
Once the area has expanded enough, the interventional radiologist will implant the stent to bridge the blocked segment and keep it open. Sometimes a second dilation with a balloon is needed to help the stent expand better.
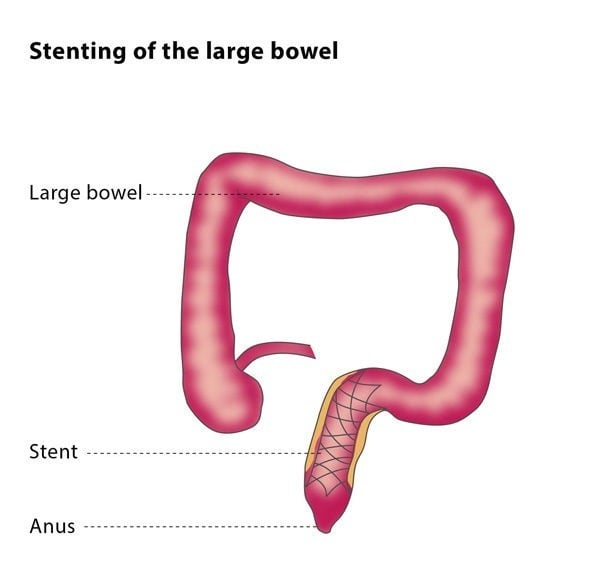
If the blockage is in your large intestine, the procedure will be performed through your anus, but otherwise the steps will be identical.
If you are being treated for a fistula, a stent covered with a membrane will be placed across the fistula before the procedure to protect it from the contents of the intestines.