
If you are on any medication which prevents blood clotting, you will stop taking it before the procedure, if possible.
You should not eat anything before the procedure. The interventional radiologist will insert a tube in your nose which will go into your stomach (called a nasogastric tube) and then will perform an ultrasound of your stomach to check the position of your liver and confirm that the tube is correctly placed.
The procedure is usually performed under local anaesthesia or moderate sedation. You may be given antibiotics to prevent infection, but this is not always necessary. You will lie on your back on the fluoroscopy table.
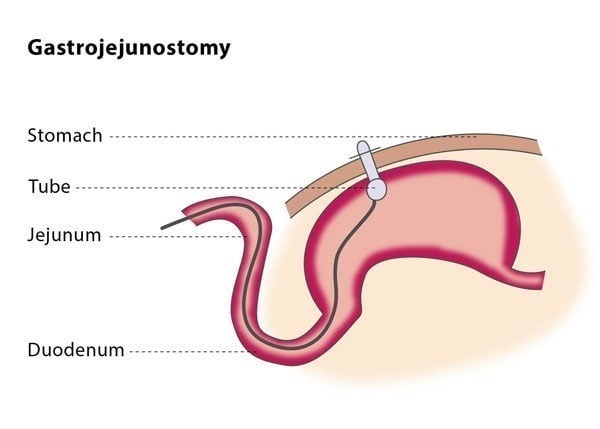
The procedure is similar to that of percutaneous gastrostomy. In most cases, you will be given a medication which temporarily paralyses the muscles in your stomach. The stomach puncture in gastrojejunostomy is aimed at the area where your stomach connects with your small intestine as this is where the tube will go.
The interventional radiologist will then insert a catheter along with a guidewire into the jejunum, which is the middle section of your small intestine. The interventional radiologist will use dilators to expand the skin opening and then insert the GJ tube. To check the proper positioning of GJ tube,the interventional radiologist will inject a small amount of contrast media (dye) through the tube so that the position of the tube tip can be confirmed using X-ray.
You will probably be required to stay in hospital overnight, although a gastrojejunostomy can also be performed as an out-patient procedure. You may experience slight discomfort at the entry point of the catheter for the first few hours following the procedure. The location of the tube will be checked daily for signs of leakage or infection. You will be allowed to eat between 8-24 hours after the gastrojejunostomy, after you have consumed 50 ml of water per hour for at least four hours without any negative effects. The T-fasteners used in the procedure can be safely removed 10-14 days after the procedure.