
If you are on any anti-coagulation or anti-platelet medication (medication which prevents blood clotting), you will stop taking it before the procedure, if possible.
You should not eat anything before the procedure. The interventional radiologist will insert a tube in your nose which will go into your stomach (called a nasogastric tube).
A gastrostomy is usually performed under local anaesthesia or moderate sedation. You may be given antibiotics beforehand to prevent infection, but this is not always necessary. You will lie on a table designed to be used in imaging procedures.
In most cases, you will be given a drug, that temporarily paralyses the muscles in your stomach. Then, air will be entered through the nasogastric tube and into your stomach. The interventional radiologist will perform a fluoroscopy of the stomach to determine the exact puncture site, which is usually over the middle part of the stomach. In some cases, such as if part of your colon or liver is in front of your stomach, the gastric procedure may be carried out using CT.
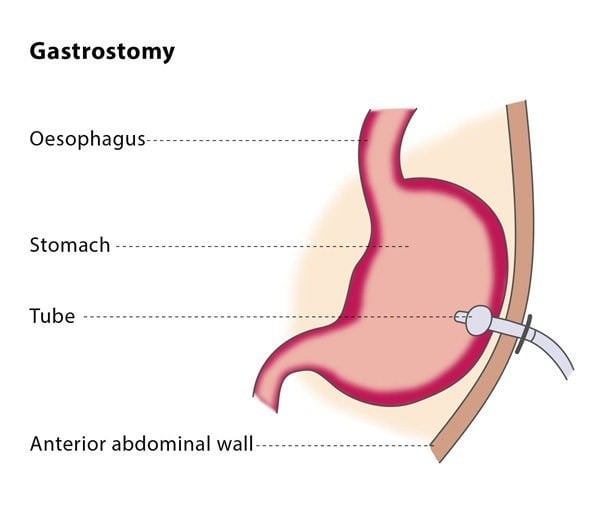
The interventional radiologist will then perform a gastropexy, which is the fixation of the anterior gastric wall to the abdominal wall by means of several anchors (T-fasteners). Thereafter the stomach will be punctured with a small needle.
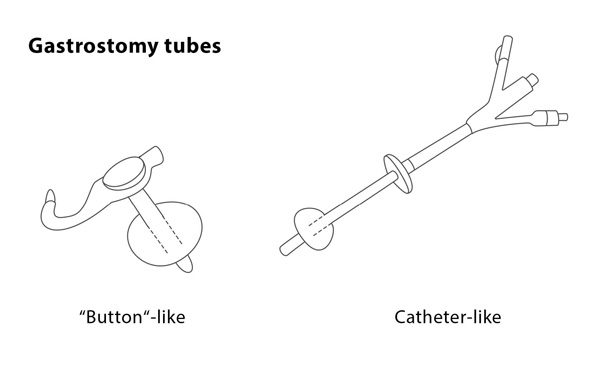
The position of the needle tip within the stomach is confirmed using air or contrast media under imaging. The interventional radiologist will then position a guidewire through the needle and into your stomach, followed by a series of dilators which will be inserted over the guidewire to expand the area around it. The gastrostomy tube will then be inserted into your stomach. It has a balloon at the end which will be inflated to keep it in place and the guidewire will be safely removed. The interventional radiologist will inject a few millilitres of contrast media through the gastrostomy tube so that the position of the tube can be checked using fluoroscopy.
You will probably be asked to stay in hospital overnight, though the procedure can in some cases be performed as an out-patient procedure. You may experience some discomfort around the catheter in the first few hours following the procedure.
The entry point for the gastrostomy tube should be checked daily for signs of leakage or infection. You will be able to begin eating again few hours after the procedure. The gastropexy anchors can be safely removed 10-14 days after the procedure.
The technical success rate of the gastrostomy procedure is very high, at around 97%.